Adolescent idiopathic scoliosis (AIS) represents over 80% of all diagnosed cases of scoliosis in children. Scoliosis can progress quickly when the skeleton is still growing or during hormonal changes.
Skeletal maturity occurs at the age of approximately 14 to 17 for females and 18 to 22 for males when the bones and spine are no longer malleable. If started young enough and depending upon maturity and magnitude of curvature, scoliosis bracing treatment can reduce the curve and Cobb angle and significantly reduce the requirement for surgery in later life.
Mild cases of scoliosis may self-correct as a child grows. However, it is important that any existing curvature is monitored closely to check progression, particularly during periods of rapid growth during puberty.
For more serious cases (Cobb angles in excess of 25 degrees) we recommend non-surgical treatment with our bespoke version of the Cheneau brace, the LOC Scoliosis Brace.
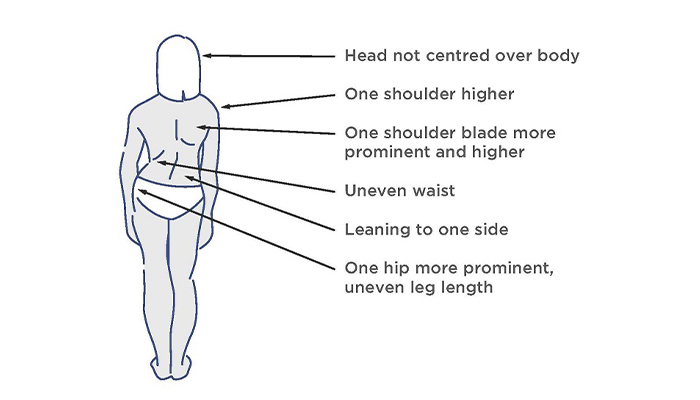
The visual signs of scoliosis
The patient pictured was diagnosed with adolescent idiopathic scoliosis at the age of 14 during a rapid growth phase. She had a thoracic curve of 35 degrees and was referred by a specialist for a spinal brace to manage her condition conservatively. After 6 weeks of wearing a bespoke Cheneau-Gensingen brace her curve in-brace had reduced to 12 degrees.

If your child has been diagnosed with scoliosis, you will naturally want to know whether the curve will get worse particularly if your child has not reached full maturity.
A number of scientific studies have established a risk factor or formula to estimate the risk of scoliosis progression for children with idiopathic scoliosis. In general, the more growing a child with scoliosis has to do; the greater the chance is that their scoliosis will get worse. As a young child’s skeleton is immature and can undergo rapid periods of growth during puberty, their scoliosis can rapidly progress during these growth spurts.
For instance, a 2017 study found that at the beginning of puberty, children with curves greater than 30 degrees had a 100% risk of progression to what is within surgical range (>45 degrees); while children with curves 21 – 30 degrees still had a 72.5% risk of progressing to that stage. (source: Charles, Yann Philippe; Daures, Jean-Pierre; Rosa, Vincenzo de; Diméglio, Alain (2006): Progression risk of idiopathic juvenile scoliosis during pubertal growth
Based on the magnitude of a curve present in a child at a particular stage of skeletal development, we can predict their likelihood of progression. Because every child is different, age does not directly correspond to a given stage of puberty, so one needs to factor in a combination of bone/skeletal age (determined by Risser sign), age, and the Cobb angle of the curve.
LOC can calculate the risk for you if you provide the following information:-
Please send the information to: [email protected], with the subject line: Scoliosis risk of progression calculation
One of our scoliosis clinicians will respond promptly and if it looks like your child does have a significant risk of curve progression, treatment options can be discussed in an initial free virtual assessment

Join The London Orthotic Consultancy in celebrating Cerebral Palsy Awareness Day on March 25th. Learn just how important expert orthotic care is in enhancing mobility, independence, and quality of life for children and adults with cerebral palsy.

Introducing the Agilik™ smart orthosis, a cutting-edge, powered knee orthotic now available in the UK through the London Orthotic Consultancy. Unlike traditional KAFOs or heavy exoskeletons, the Agilik™ provides dynamic knee assistance and offers real-time support, reducing fatigue and improving posture. This pioneering, modern technology can help children and adults with lower limb weakness walk more efficiently and naturally. We are honoured to be selected as the exclusive paediatric specialist centre in the UK for the Agilik™ device.

When Sophie noticed her baby Max had a persistent flat spot on his head, she was told it would resolve naturally—but it didn’t. Seeking a second opinion led her to the London Orthotic Consultancy, where Max was diagnosed with severe plagiocephaly.

A little more than four years after the LOCband Lite's launch, we're proud to have successfully treated our 250th helmet therapy patient at our Romford clinic using our cutting-edge 3D-printed cranial band. After five months of treatment, her final scan showed that her asymmetry had decreased from 12 mm to 3 mm.

Sky News published an article this month quoting scientists at Southmead Hospital who claimed there was a lack of research into flat head syndrome and its treatment with cranial remoulding (helmet) therapy. This is our response.

With our non-surgical treatment plan, Alex achieved 100% chest correction in just two years. His treatment involved a combination of dynamic chest compressor and vacuum bell therapy treatment to address his pectus excavatum and rib flaring.

Learn how a custom carbon fibre AFO helped Gill regain mobility and comfort despite complex challenges from shin bone (tibia) removal. We created a truly tailored orthotic solution made from pre-preg carbon fibre at our Cambridge clinic.

Discover how bespoke orthotics and the OSKAR program with Elaine Owen transformed Archie’s life with cerebral palsy quadriplegia, helping him avoid a wheelchair and achieve greater mobility.