Club foot, or clubfoot, is the general name given for a medical condition called congenital talipes equinovarus (CTEV). Congenital means that you’re born with the condition, which can occur in one or both feet. It is quite common, occurring in around one in every 1,000 babies born in the UK.
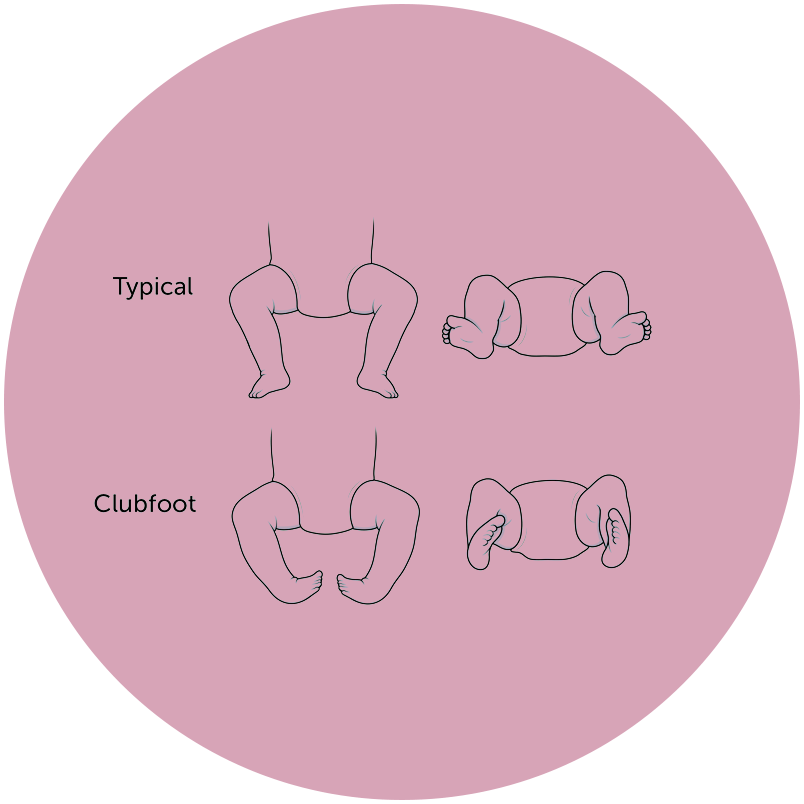
The affected foot will look like it’s rotating internally at the ankle, with the foot pointing down and inwards. The soles of the feet face backwards. If left untreated, people with club feet often appear to be walking on their ankles or the sides of their feet.
Young babies are naturally flexible, and we can use some of that to correct club foot. There are stages to that process and most cases respond well to correction using the Ponseti method (see question four) followed by a long period of maintenance using what is known as the ‘boots and bar’ approach.
LOC does not carry out the Ponseti method directly. Instead, we see patients who are referred to us or who have already been seen by club foot and Ponseti experts. Typically, we work with patients in that final boots and bar stage. However, we are pioneering the use of a different brace, known as the Cunningham Brace (see question six).
We are the only clinic in the UK and Europe offering Cunningham Brace treatment and we will only proceed if our clinical judgement is that your baby’s condition has been fully corrected by Ponseti treatment.

The Ponseti method involves manipulation and repeated weekly casting for about five to eight weeks. After that, a small procedure called a tenotomy is carried out under local anaesthetic to lengthen the tight heel cord – known as the Achilles tendon – in the back of your ankle.
The treatment follows very strict, well-understood protocols and is the gold standard in corrective treatment for club foot. Indeed, the procedure is used and endorsed by Great Ormond Street.
What is the ‘boots and bar’ approach?
This is the second, long-term stage of treatment, once the Ponseti method is complete. Just as it sounds, this treatment involves wearing a pair of special boots – full time – for the first three months after treatment and then overnight until the child is around four or five years old. Both feet are essentially strapped together, which is an enormous undertaking meaning that compliance is critical for success. While success rates are high, we know a lot of parents find the process very challenging. That’s why we work with the Cunningham Brace.
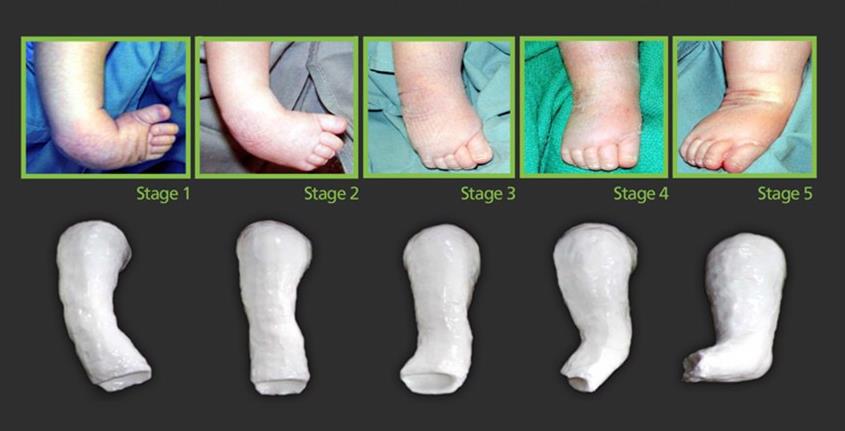
Above: Casting after the operation - Image courtesy of Cunningham Prosthetic Care
The Cunningham Brace was designed by Jerald Cunningham, who runs his own clinic in the US. It works using a firm strap around the thigh and a spring that holds the brace up against the bottom of the foot. This means that the brace is always gently stretching your baby’s foot into the correct position, in a similar way that a therapist applies manipulation.
Jerald developed the brace at the request of an orthopaedic surgeon and colleague who saw how distressing the boots and bar process was for many children and parents. Jerald has worked on the design for more than 10 years, tweaking as he goes, based on x-ray evidence after every patient fitting.

Above: Child wearing Cunningham brace - Image courtesy of Cunningham Prosthetic Care
The big difference is that the Cunningham Brace is flexible and only fitted to the affected leg. This allows for the sort of dynamic movement you’d expect in babies, such as crawling, rolling and standing. Greater activity helps build a more developed muscular system – particularly calf muscles. Anecdotally we’ve seen a lot more symmetry in calf muscles using the Cunningham Brace than boots and bar. And because it’s a different kind of mechanism we don’t have to strap the feet up so tightly, which reduces issues such as blistering on the legs.

At your first appointment, we will take measurements and fit your child with their first Cunningham Brace. We’ll show you how to put the brace on and take it off and book you in for a review a week later. We then schedule a series of reviews as your child grows to check progress and ensure that your child is maintaining the correction. This can be done in the clinic or virtually via a system like Skype. There are lots of simple things we can adjust to encourage correct development.
The Cunningham Brace is made from a series of measurements that we can either take in the clinic or help you to take during a virtual appointment. We hold a range of Cunningham braces in stock that we can adapt to the correct size and foot type of your baby. This process normally takes a few hours unless your child has a size that is out of the normal range or we do not have it in stock.

It depends on your child and the complexity of their case. On average, though, we’ll be looking to review your baby’s progress once a month over the course of treatment.
Treatment lasts about two years – this is around one third of the time other methods require. In the first year, your baby will wear the brace for 23 hours a day – compared with boots and bar which can only be done for three months. This means we can help correct your baby’s foot while their tissue and bones are at their softest and most compliant. Once your baby is standing, they will only wear the brace during night-time and naps.
The exact number will depend on your child and their condition, but typically a child will only need to wear two to three braces over a two-year period. The first for about six months, then a year each for the second and third.

Very often parents contact us before their baby is even born, having discovered the club foot on a scan. However, they first need to go through the Ponseti method with their consultant and then be triaged by a specialist physiotherapist before we can start treatment.
No problem. Often parents come to us after they’ve tried persevering with the boots and bar treatment for a few months. It may change our treatment plan a little and your child might need treatment for a bit longer, but the process will essentially be the same.
The cost of treating club foot depends on whether your child will need one or both legs braced. You can find all the information you need on our club foot treatment pricing page.

At the moment we can fit the brace at our clinics in Kingston-upon-Thames and Bristol; in addition, we can do follow up appointments at our Manchester clinic. There is a certain amount we can do virtually, but your first fitting would need to be done in person.

If your patient has asked you for more information about club foot treatment or the Cunningham Brace, our director Sam Walmsley would be happy to speak with you directly to explain the process. We can also offer your team an online presentation. Contact the LOC team if you’d like to know more.

The Ponseti method was only introduced in the UK in the late 1990s, which means there are lots of adults living with the long-term impact of untreated club foot. The good news is that many of the common problems that adults experience can be treated effectively with orthoses. Take a look at our treatment for adults with club foot page for more information.

If you would like to talk to us about your baby’s club foot and Cunningham Brace treatment, please don’t hesitate to get in touch via our contact form or by calling us on 020 8974 9989.
Daisy was X-rayed and diagnosed with mild scoliosis of nine degrees. They also confirmed that she had pectus carinatum but advised that, as they considered this a cosmetic issue, we should simply monitor it and take no further action” ... continue reading ...
Recently we had a 14-year-old pectus patient who attended The London Orthotic Consultancy for treatment for his pectus carinatum inferior with rib flaring after only being offered surgical solutions on the NHS ... continue reading ...
Jamie consulted his GP and was told about the option of surgery but was soon put off by the risk of scarring and lengthy recovery time. It was while on a beach holiday - and feeling particularly self-conscious ... continue reading ...

Join The London Orthotic Consultancy in celebrating Cerebral Palsy Awareness Day on March 25th. Learn just how important expert orthotic care is in enhancing mobility, independence, and quality of life for children and adults with cerebral palsy.

Introducing the Agilik™ smart orthosis, a cutting-edge, powered knee orthotic now available in the UK through the London Orthotic Consultancy. Unlike traditional KAFOs or heavy exoskeletons, the Agilik™ provides dynamic knee assistance and offers real-time support, reducing fatigue and improving posture. This pioneering, modern technology can help children and adults with lower limb weakness walk more efficiently and naturally. We are honoured to be selected as the exclusive paediatric specialist centre in the UK for the Agilik™ device.

When Sophie noticed her baby Max had a persistent flat spot on his head, she was told it would resolve naturally—but it didn’t. Seeking a second opinion led her to the London Orthotic Consultancy, where Max was diagnosed with severe plagiocephaly.

A little more than four years after the LOCband Lite's launch, we're proud to have successfully treated our 250th helmet therapy patient at our Romford clinic using our cutting-edge 3D-printed cranial band. After five months of treatment, her final scan showed that her asymmetry had decreased from 12 mm to 3 mm.

Sky News published an article this month quoting scientists at Southmead Hospital who claimed there was a lack of research into flat head syndrome and its treatment with cranial remoulding (helmet) therapy. This is our response.

With our non-surgical treatment plan, Alex achieved 100% chest correction in just two years. His treatment involved a combination of dynamic chest compressor and vacuum bell therapy treatment to address his pectus excavatum and rib flaring.

Learn how a custom carbon fibre AFO helped Gill regain mobility and comfort despite complex challenges from shin bone (tibia) removal. We created a truly tailored orthotic solution made from pre-preg carbon fibre at our Cambridge clinic.

Discover how bespoke orthotics and the OSKAR program with Elaine Owen transformed Archie’s life with cerebral palsy quadriplegia, helping him avoid a wheelchair and achieve greater mobility.


