Scoliosis is the medical term that describes the abnormal twisting and curvature of the spine. It occurs most often during the growth spurt just before puberty. It affects around three to four children in every 1,000 in the UK and is most typically seen in children between the ages of 10 and 15. It is also more common among females than males.
Since LOC opened its Scoliosis clinic in 2017, we have treated a broad age range of patients from 3-year-olds to 80-year-olds.
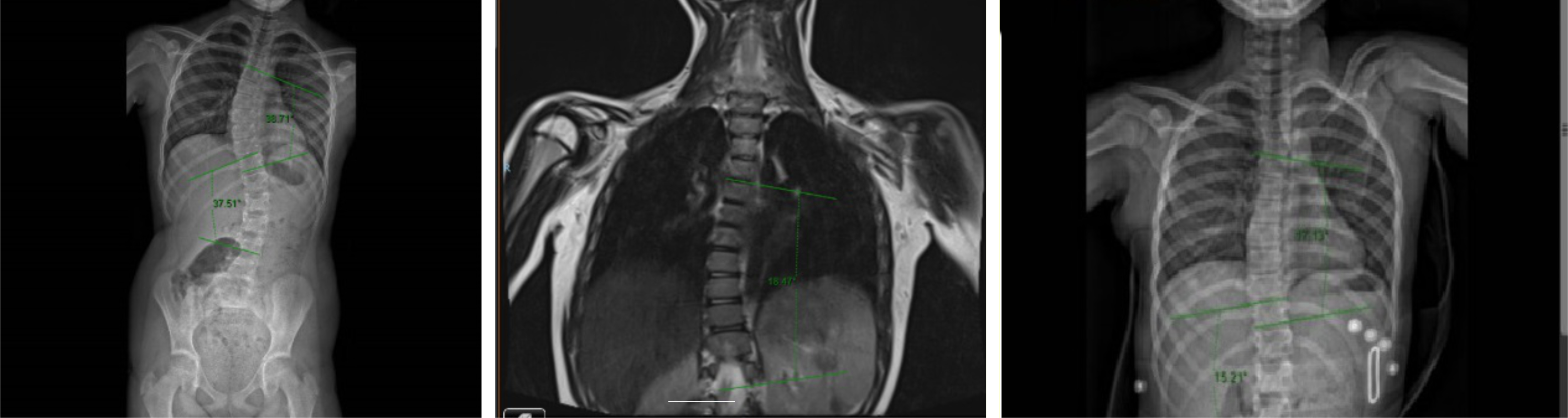
Even those with severe scoliosis, where the Cobb angle is in excess of 40 degrees, have responded well to the combination of bracing with the Cheneau-Gensingen brace and a physiotherapy programme that follows the principles of Schroth physiotherapy.
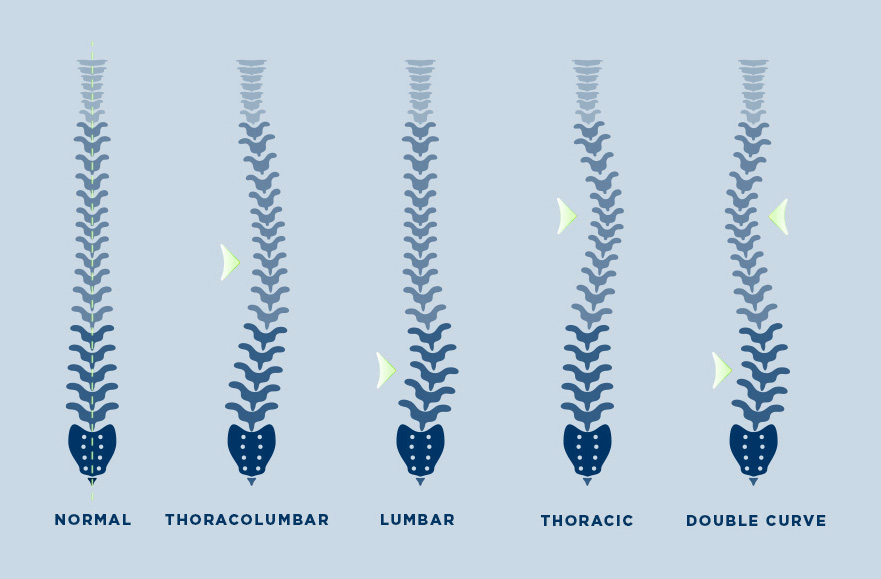
Classification of scoliosis curves
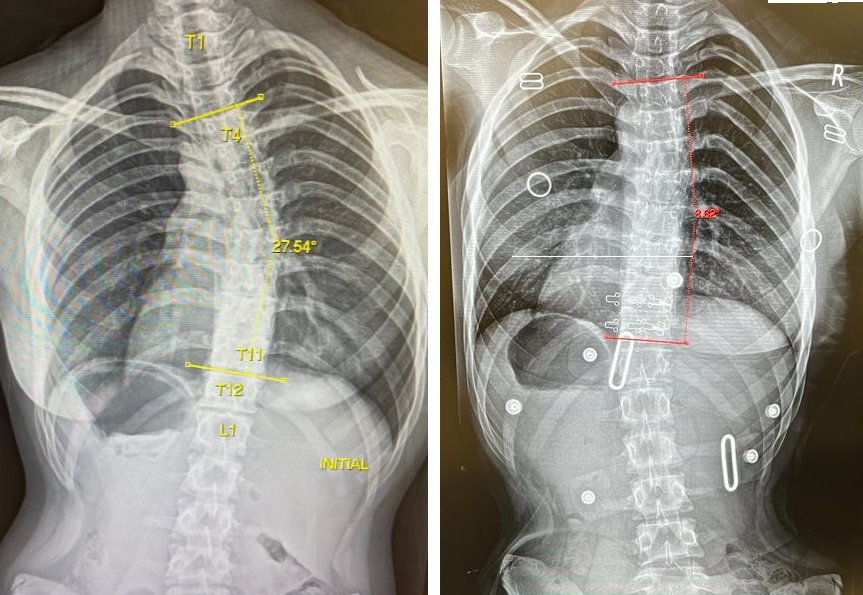
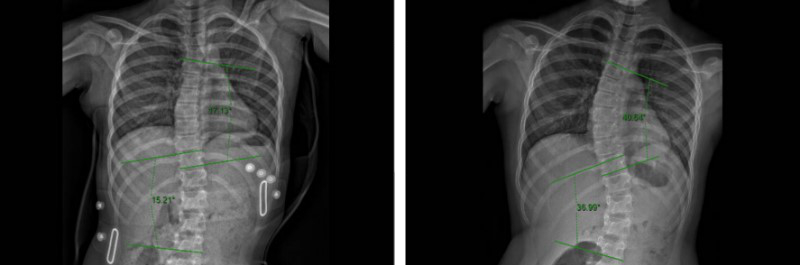
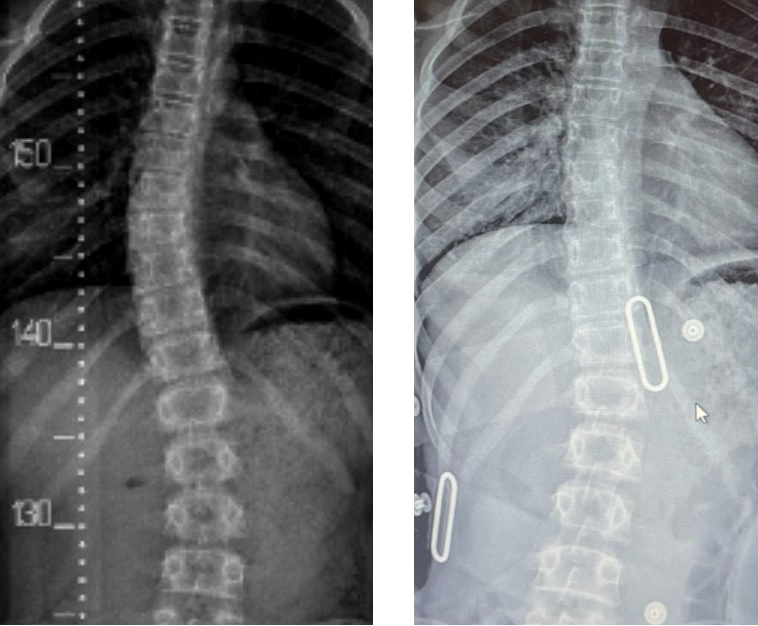
Before & After
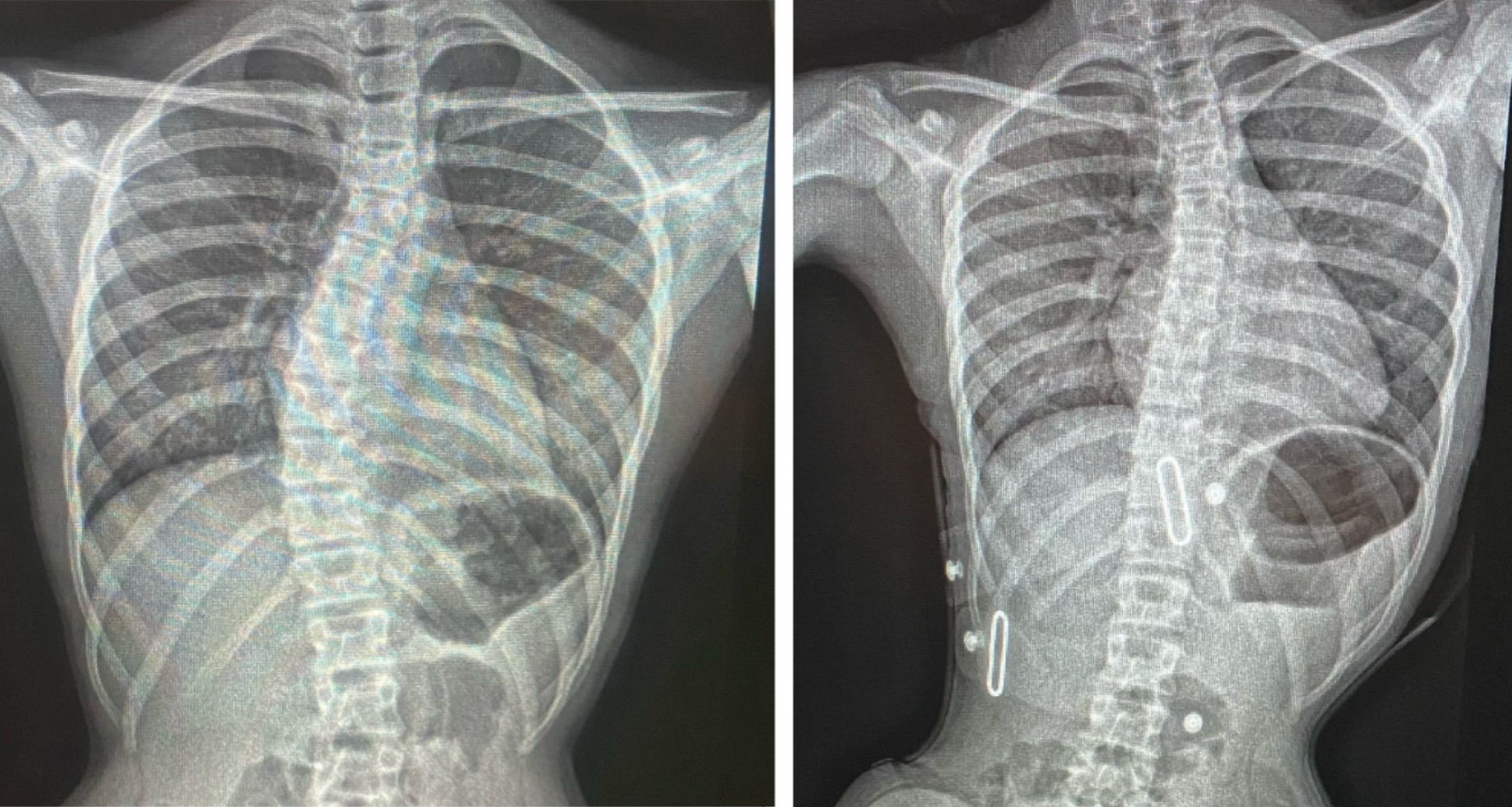
Before & After
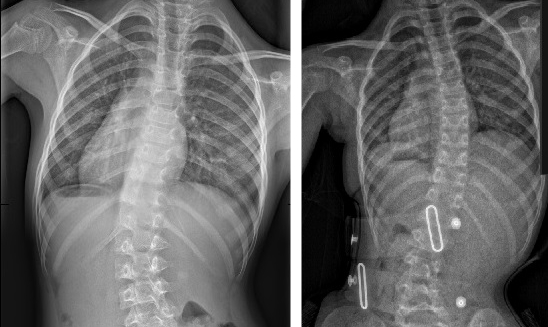
Before & After
Before & After
Before & After
Before & After
Before & After
Before & After
Before & After
Before & After
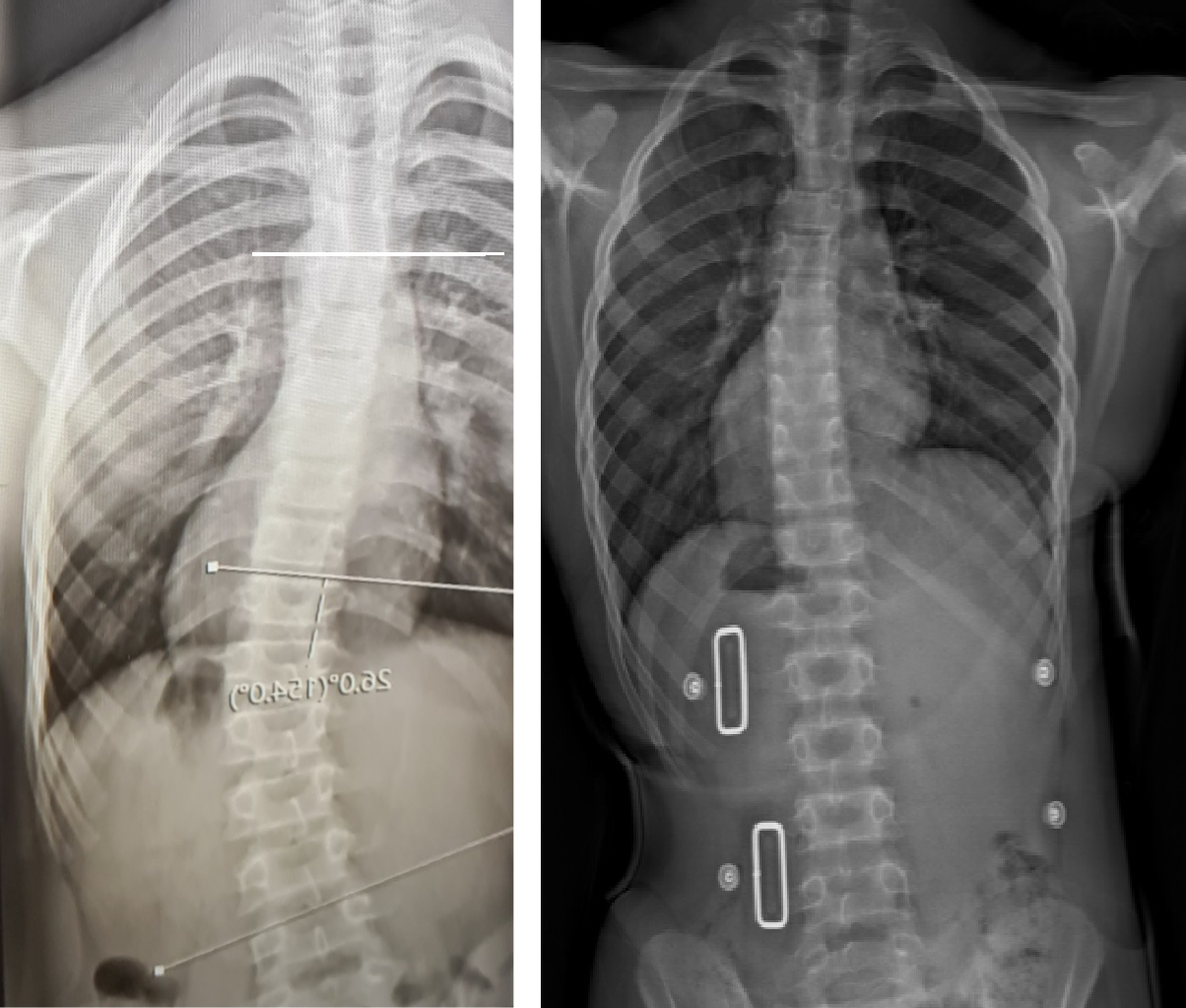
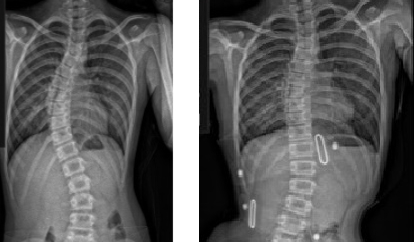
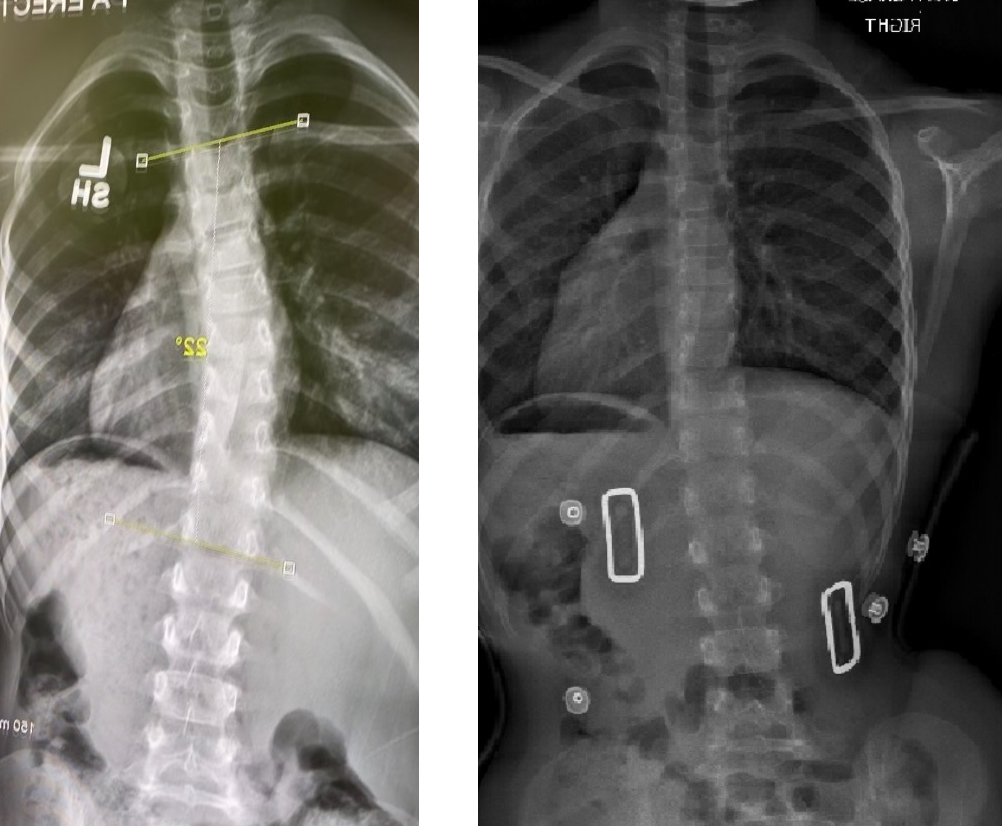
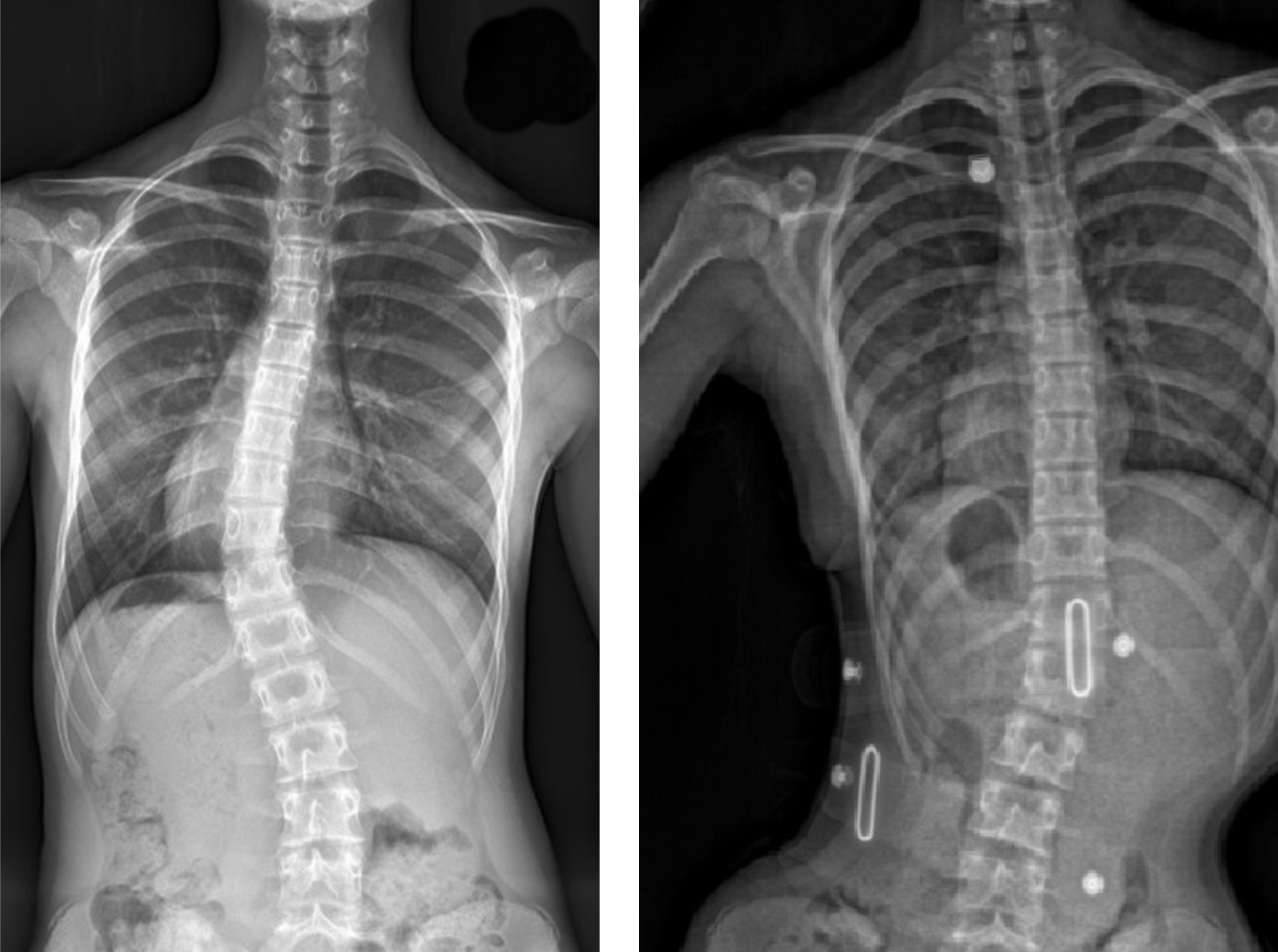
As of September 2022, these are some of the in-brace x-ray results from our LOC Scoliosis Brace

LOC is pioneering the non-surgical treatment of scoliosis through back bracing with the LOC Scoliosis Brace and specialist Schroth Treatment physiotherapy as spinal surgery is extremely invasive and can lead to complications.

The LOC Scoliosis Brace takes a three-dimensional approach to scoliosis treatment. This type of bracing is regarded by many scoliosis clinics around the world as the preferred alternative to surgery, since it has been proven to reduce Cobb angles and improve posture.

Our bespoke scoliosis treatment can be combined with a comprehensive physiotherapy programme that adheres to the principles of the world-renowned Schroth treatment.
Our treatment package price includes all reviews and on-site adjustments of the brace by our certified orthotists.

There may be cancellations or delays to your child’s spinal surgery for several reasons. At LOC, we are here to assist where possible. Using our corrective LOC Scoliosis Brace, we can halt the curve's progression, balance posture and reduce any back pain.

Our scoliosis treatment recommendations are based on the severity of the Cobb angle and the age of the patient. If the Cobb angle is over 25° it is likely that we will recommend a LOC Scoliosis Brace combined with Schroth physiotherapy. Our treatment is customised for all age groups, juvenile, adolescent and adult.

Kyphosis causes pain if excessive or if in the wrong place such as the lower back.
Our bespoke physiotherapy programme can improve muscle lengths & spinal extensor strength, reducing postural pain.
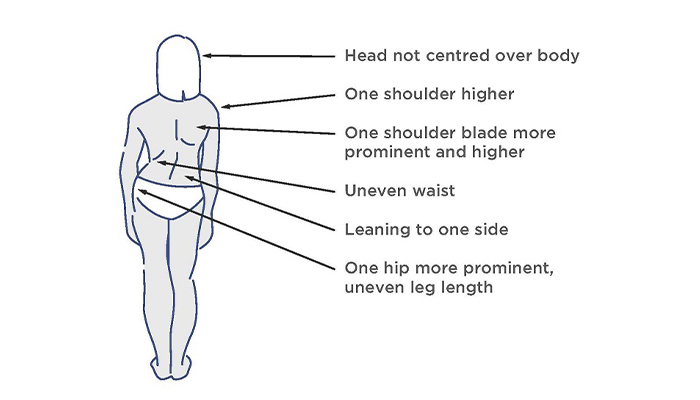
Scoliosis may first be noticed by a change in the appearance of a child’s back. Symptoms can include:
Each scoliosis curve is unique. The spine may curve to the left or right and it can happen in different parts of the spine. If it is in the chest area it is called ‘thoracic’ scoliosis, while if it is the lower part of the spine it is called ‘lumbar’ scoliosis. It is also possible to have two curves; this is called a double curvature and the spine may look like an ‘S’ shape from behind. It is further possible to have more compensatory curves at the top and bottom of the spine.
As scoliosis is a three-dimensional condition and the spine is always trying to compensate there are numerous potential curve variations. However, the most common curve is the right thoracic curve.
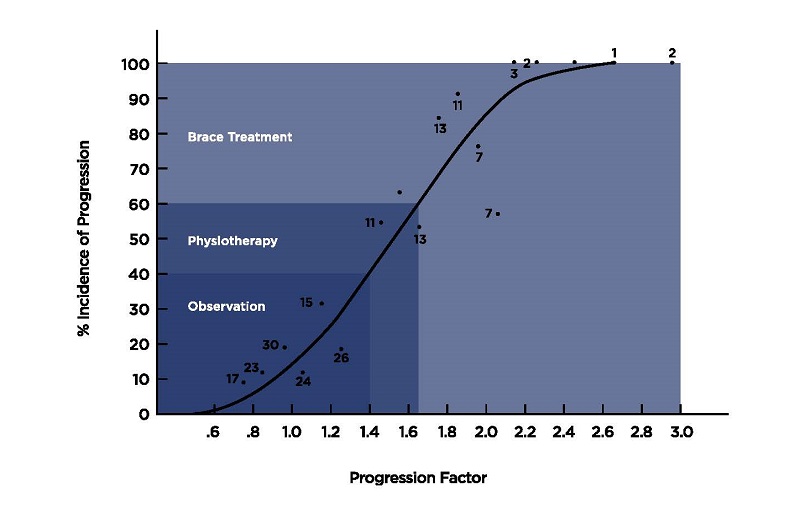
At the moment you may find it difficult to get a referral to your local hospital, we can provide clinical assessments and refer your child for any necessary back x-rays or scans required. These scans will help us determine the progression factor. This is the incidence of progression of untreated idiopathic scoliosis according to the formula by Lonstein and Carlson (see graph); this considers the severity of the curve and the skeletal maturity of the patient.
A patient’s treatment can involve one or all of these elements: observation, specialist scoliosis physiotherapy and bespoke back bracing. The correct prescription and combination of these elements will be determined by one of our team of specialist scoliosis clinicians. At the patient’s initial consultation, the clinician will look at posture, the exact nature of the curve and its flexibility and will also assess the pain associated with the condition. The skeletal maturity and age of the individual will also affect the recommended treatment plan, as described above.
Scoliosis can progress quickly when the skeleton is still growing or during hormonal changes so if you are concerned about your child please contact us.
References:
At the initial consultation, we will conduct a detailed clinical assessment to assess posture/leg length/progression factor of the curve/flexibility of the body and then discuss the most appropriate treatment. If you have already been diagnosed with scoliosis you will need to bring with you a recent X-ray of your spine. The existence of scoliosis is established by measuring the Cobb angle of the spinal curves. The Cobb angle was first described in 1948 by Dr John R Cobb, an American orthopaedic surgeon. A Cobb angle of 10° is regarded as the minimum angulation to define scoliosis.
We use a scoliometer to measure the angle of trunk rotation. This is a small non-invasive device that is placed over the spine while the patient being measured is in a forward bending position. As it provides a reading in degrees, it is important not to confuse the Cobb reading with a scoliometer reading. The scoliometer is a useful tool for monitoring our patients while reducing the need for x-rays.
Our scoliosis treatment recommendations will be based on the severity of the Cobb angle and the age of the patient. This allows us to calculate the risk of progression and determine the most appropriate conservative management for each patient. We also factor in the individual’s lifestyle and symptoms.

The criterion for treatment is based on the patient’s Cobb angle:
Alex has been in full-time bracing, managing around 22 hours a day, due to the comfort of the brace. This has been combined with daily Scoliogold exercises provided by Scoliosis SOS, our partner in providing non-surgical treatment for scoliosis ... continue reading ...
In year three of school, Daisy’s mum, Sara, noticed something amiss with her posture. “I’m an orthopaedic physiotherapist, so I recognised that something was not quite right and suspected that we might be looking at scoliosis,” she explains ... continue reading ...
LOC recently heard from one of our young patients, Beau, who was diagnosed in 2020 with juvenile idiopathic scoliosis. Beau has embraced her treatment programme wholeheartedly. Her positive outlook and ‘can-do’ attitude are inspiring ... continue reading ...
Ariana was examined by LOC clinicians who checked for spinal rotation using a scoliometer device that measures how much a rib hump protrudes - known as ‘angle of trunk rotation’ (ATR) ... continue reading ...
It is fair to say that Venetia had been through the mill before she came to see us in March. It started about 3 years ago when Venetia kept getting bad cramps at night. Having rejected the quinine prescription suggested by her GP ... continue reading ...
LOC first met 11-year-old Yasmin after she found out she had adolescent idiopathic scoliosis quite by chance; an X-ray taken for a chest complaint revealed she had abnormal twisting and curvature of the spine ... continue reading ...
We talk to the father of one of our scoliosis patients Ricarda, a thirteen-year-old horse rider and regional kickboxer, about her experience with adolescent idiopathic scoliosis and treatment with the Cheneau-Gensingen brace ... continue reading ...
Motivated Angelina is a thirteen-year-old scoliosis patient currently going through scoliosis treatment, here her mother Paola talks to us about her scoliosis journey and her experience with the brace ... continue reading ...
Victor the Robot, our new Computer Numerical Control milling machine, in action! Victor is noisy, but he’s transforming our ability to design and manufacture orthotic devices at our Kingston-upon-Thames clinic.
Manufactured by Rodin4D, Victor is capable of milling complex ergonomic shapes, meaning that we can now potentially assess a spinal orthotic patient, manufacture the orthosis and have it fitted, all in the space of a day. Victor can do everything we need to do for our patients, in-house and in the shortest time possible with no compromise on quality.

Join The London Orthotic Consultancy in celebrating Cerebral Palsy Awareness Day on March 25th. Learn just how important expert orthotic care is in enhancing mobility, independence, and quality of life for children and adults with cerebral palsy.

Introducing the Agilik™ smart orthosis, a cutting-edge, powered knee orthotic now available in the UK through the London Orthotic Consultancy. Unlike traditional KAFOs or heavy exoskeletons, the Agilik™ provides dynamic knee assistance and offers real-time support, reducing fatigue and improving posture. This pioneering, modern technology can help children and adults with lower limb weakness walk more efficiently and naturally. We are honoured to be selected as the exclusive paediatric specialist centre in the UK for the Agilik™ device.

When Sophie noticed her baby Max had a persistent flat spot on his head, she was told it would resolve naturally—but it didn’t. Seeking a second opinion led her to the London Orthotic Consultancy, where Max was diagnosed with severe plagiocephaly.

A little more than four years after the LOCband Lite's launch, we're proud to have successfully treated our 250th helmet therapy patient at our Romford clinic using our cutting-edge 3D-printed cranial band. After five months of treatment, her final scan showed that her asymmetry had decreased from 12 mm to 3 mm.

Sky News published an article this month quoting scientists at Southmead Hospital who claimed there was a lack of research into flat head syndrome and its treatment with cranial remoulding (helmet) therapy. This is our response.

With our non-surgical treatment plan, Alex achieved 100% chest correction in just two years. His treatment involved a combination of dynamic chest compressor and vacuum bell therapy treatment to address his pectus excavatum and rib flaring.

Learn how a custom carbon fibre AFO helped Gill regain mobility and comfort despite complex challenges from shin bone (tibia) removal. We created a truly tailored orthotic solution made from pre-preg carbon fibre at our Cambridge clinic.

Discover how bespoke orthotics and the OSKAR program with Elaine Owen transformed Archie’s life with cerebral palsy quadriplegia, helping him avoid a wheelchair and achieve greater mobility.







