
04 April 2018
Learning that your baby has flat head syndrome can be daunting – especially with the sea of misinformation available on the internet. So, as the 4th of April is World Plagiocephaly Awareness Day, we thought we'd make it easier by debunking 9 common myths about the condition, hoping to put your worries to rest and set the record straight.
It can be quite traumatic for parents when they discover an abnormality in their baby’s head shape – and the tendency is to blame themselves. Many parents experience a “this is my fault” moment, which couldn’t be further from the truth.
Many factors can cause flat spots to develop; most of the time they are completely unavoidable. They can be caused naturally, either during pregnancy due to a baby’s position in the womb or because the baby has problems with its neck and shoulder muscles from torticollis, or ‘wry-neck’, causing their head to naturally revert to one position – placing more pressure on one side of the head.
Most often, babies are born with a normal head shape which gradually flattens as a result of the position they spend most of their time in. Head shape can also be altered by external forces like spending prolonged periods in car seats, buggies or hard mattresses.
It has been well documented that the ‘Back to Sleep’ campaign to prevent cot death has caused an increase in flat head syndrome cases. When a baby is young their skull is malleable, so constantly sleeping on their backs – the supine position – can increase their risk of flat head syndrome.
As a parent you should never blame yourself – UK government guidance strongly recommends that infants sleep on their backs to decrease the risk of cot death.
Naturally, parents often worry that the helmets used to treat flat head syndrome would be painful for their child. This is however not the case – the inside of the LOCband helmets are made of a soft foam layer and apply very gentle pressure on the most prominent areas of the head, whilst providing ample space for the flat, dented areas to grow naturally into position.
This process is completely non-invasive and will not put the baby in any discomfort. Our helmets are custom made for each child and are also adjusted frequently to aid normal growth of the head into a more symmetrical shape.
Read about Baby Amrit's story and his first plagiocephaly appointment
Many parents worry that their baby will develop sores as a result of the helmet, however, this is not the case. Every baby going through LOCband treatment is closely monitored with the helmet being reviewed and adjusted accordingly – preventing any rubbing which could cause sores.
Additionally, cranial remoulding helmets are recognised and heavily regulated by the Medicines and Healthcare Products Regulatory Agency (MHRA), the UK medical products regulator – meaning they are completely safe for use.
It’s true that flat head syndrome is regarded as a cosmetic issue by the NHS. By definition, this means that your baby is not usually at risk, and there is no fundamental disease present. However, that fails to take into account the impact cosmetic issues can have on a person’s self-esteem and social development. Because treatment is only viable up to the age of 18 months, when the skull hardens, the opportunity can be missed to do anything about it, particularly if the deformity becomes more pronounced in later life. It’s possible that they may feel picked on by their peers for the abnormal shape of their head, making them feel less confident.
Practically, it may be difficult to wear glasses or protective helmets for sport or work. An adult who experienced severe plagiocephaly as a child may be less inclined to have short hairstyles and feel self-conscious about their appearance.

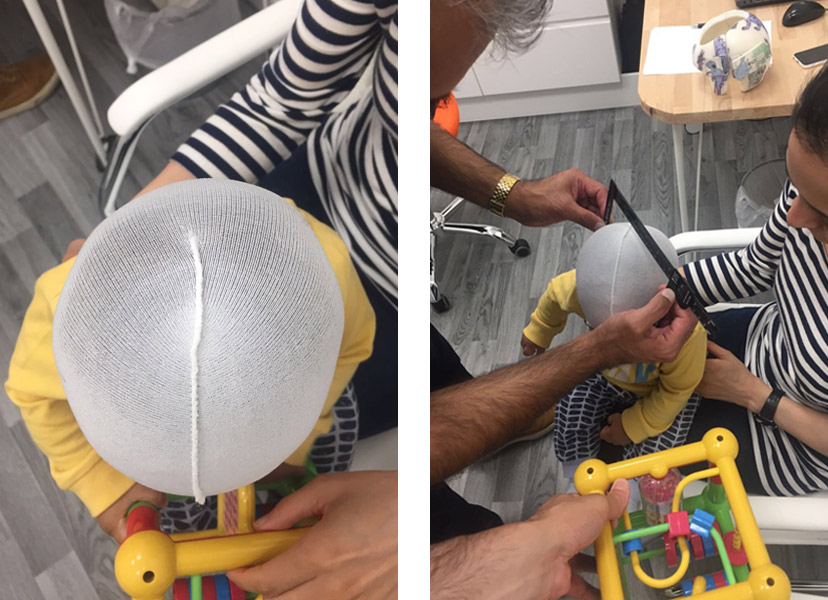
Above: Baby Amrit being scanned
If you suspect that your child’s head is abnormally shaped and you visit a doctor, they will advise you to try repositioning techniques and that it will correct itself naturally.
Whilst this has proved successful for very mild cases of flat head syndrome, many babies find it difficult to comply with repositioning and so it does not correct itself and will inevitably require treatment later down the road. Previous studies have proven that deformational asymmetries will not correct on their own without the intervention of some kind.
If a cranial remoulding helmet is a way to go, the sooner the better; the younger a baby is, the more malleable its head will be, and as they grow older, their skulls harden and become less responsive to helmet treatment.
The ideal age for LOCband treatment is between four and seven months – however, it is still applicable to babies of up to 18 months, when the soft spots on the head are no longer malleable.
Many parents often worry that they are alone in this situation, however, the reality is that flat head syndrome is much more common than you think – and many families will be going through exactly the same thing.
The NHS states that around 1 in 5 babies will develop it at some point in their early lives – making it anything but rare. The key is to notice it early and have the condition diagnosed and treated whilst your baby is still able to respond to treatment.
There is absolutely no risk of this – empirical research has been carried out and shows that helmet therapy poses no risk to development. The only scenario in which helmet therapy would be inadequate, if they are young enough, is if the helmet is not worn for the designated 22-23 hours a day as a result of poor parental compliance.
Many parents also worry that the condition will return to normal after their child stops wearing the helmet. Neither is this a reason for worry – once the skull reaches maturity and the fontanelles are fused, the skull cannot change shape without surgical intervention.

As the NHS defines flat head syndrome as a cosmetic issue, this means they do not designate funding to treat it. The exception to this rule is Bristol Children’s Hospital. However, they use a general anaesthetic on the baby in order to make the cast for the helmet. In the rest of the UK, to get treatment, parents have to look to private specialists who can carry out the treatment. There are many charities that offer funding support for parents to pay for treatment, such as Tree of Hope and Headstart4Babies.
Perhaps the greatest myth of all. A retrospective report of 4,000 babies showed that 94.4% of the infants who started in the helmet-treated group achieved full correction in the asymmetry of their head shapes, as did 96.1% of those who were transferred from the initial repositioning group into the helmet-treated group.
At LOC, every baby that has completed the LOCband treatment has achieved measurable improvements to their head shape. We have successfully treated thousands of babies with positional plagiocephaly over the last decade.
If your baby’s head shape is causing you to worry, you can upload photos of your baby’s head to our Flat Head Diagnosis Form and one of our skilled orthotists will respond within 24 hours. If you already know your child has plagiocephaly, we offer a free consultation to discuss treatment options.

This is very much dependent on how fast your baby is growing. The faster the growth, the more frequently your baby will be seen so that the helmet can be adjusted. In general, reviews will happen at two to four-week intervals.
The price of treatment covers:
Yes - All babies that have completed their course of treatment with us have achieved a measurable improvement in head shape. However, you don’t have to take our word for it.
Recent independent research conducted by a University Hospital in Germany has endorsed the treatment for babies with moderate or severe plagiocephaly.
A larger, retrospective study has just been published that found complete correction was achieved in 94.4% of babies treated with helmet therapy.
The results were conclusive: repositioning achieved acceptable correction in 77.1% of cases, but 15.8% were moved onto helmet therapy because re-positioning was not working. Meanwhile, 94.4% of the infants who started in the helmet-treated group achieved full correction, as did 96.1% of those who were transferred from the repositioning group into the helmet-treated group.
Further information can be found on our Plagiocephaly Research page.
If your baby has a temperature or a fever due to illness you must remove the band. The band can be put back on once the temperature has returned to normal.
The optimum age for treatment is between four and seven months.
This is because the skull is most malleable at this age and improvements to head shape tend to take less time and are more dramatic. That is not to say that helmet therapy should be ruled out if the baby is older than seven months. Routinely, babies up to the age of 16 months can be treated very successfully.
The cut off age is around 18 months when the fontanelles (soft spots on the head) are no longer malleable. As babies grow and develop at different rates, it is always worth checking if you are not sure. There have been cases where a baby’s fontanelles have not fused yet by the age of 18 months, who have achieved successful, but less-marked results with cranial remoulding therapy.
Torticollis is a condition in which a tight or shortened muscle in one side of the neck causes the head to tilt or turn to one side, resulting in the infant resting its head in the same position. In 2013, we analysed the data from all first appointments in our Kingston clinic and found that 20% of the babies examined had some kind of neck condition that was causing head immobility.
The clinics and clinicians that provide this treatment in the UK will have received similar training and experience. However, we are the only clinic that manufactures its own helmet and our clinicians are closely involved with the process for each individual helmet that we produce.
In addition, we do not restrict review appointments to a set number, we are extremely flexible and respond to individual parents' needs so that the best outcome can be achieved for each baby.
The LOCband is non-invasive and works by applying gentle, constant pressure over the areas of the baby’s skull that are most prominent while allowing unrestricted growth over the flattened areas. The band consists of a soft foam layer inside a thermoplastic shell. As the baby grows, the band will be adjusted frequently to gently guide the skull into a more symmetrical shape.